AI Deepfakes and Deskilling in Healthcare Are Reshaping Hospitals
AI adoption hospitals, AI hallucinations, AI in healthcare, AI medical scribes, artificial intelligence ethics, clinical decision support, clinical skills, deepfakes in medicine, deskilling, healthcare AI risks, medical AI governance, medical technology, patient safety, physician burnout, Wolters Kluwer survey
Carolyn Stinnett
0 Comments
7 Alarming Ways AI Deepfakes and Deskilling in Healthcare Are Reshaping Hospitals
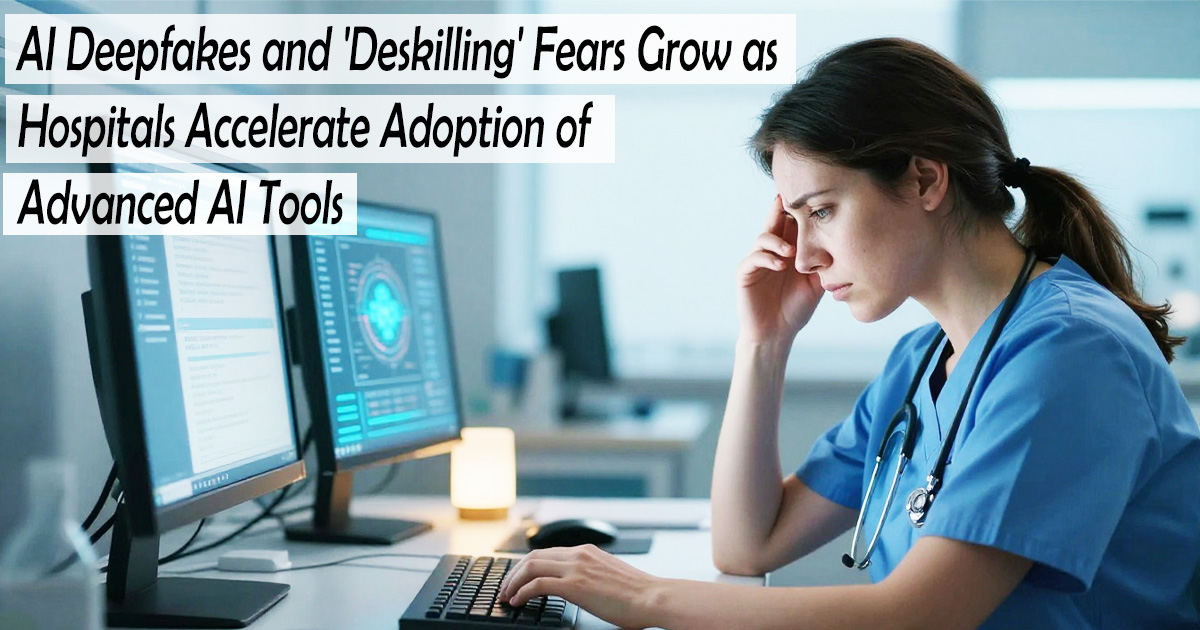
AI Deepfakes and ‘Deskilling’ Fears Grow as Hospitals Accelerate Adoption of Advanced AI Tools
AI Deepfakes and Deskilling in Healthcare : The pace is dizzying. Just a few years ago, mentioning AI in a hospital got you puzzled looks. Now, in any ward, you’ll find doctors dictating into AI scribes, nurses querying LLMs for drug interactions, and clinical decision support tools offering second opinions. A recent Wolters Kluwer Health survey found nearly three-quarters of doctors and 70% of nurses use AI at least weekly — a leap from about 4 in 10 just a year earlier. That speed brings two fears: AI-generated deepfakes eroding public trust, and a more personal concern that leaning too hard on the technology could slowly dull clinical judgment. Both are real. Both deserve plain talk.
The Spread of AI Tools
This isn’t tinkering anymore. Over half of doctors now use AI to summarize medical literature or crunch data. About 44% use AI scribes that listen to patient encounters and draft clinical notes on the spot. Nurses lean on the tech for scheduling and care-plan suggestions too. The rapid adoption of these technologies has made AI Deepfakes and Deskilling in Healthcare a growing topic of discussion among medical professionals.
Seasoned doctors who once swore by handwritten notes now admit they’d hate to go back. But they also tend to read every AI-generated line, line by line. That vigilance is the crux. The same survey found that while clinicians embrace AI, 74% said losing critical thinking or decision-making ability would be one of the greatest risks. They’re not wrong to worry. Concerns surrounding AI Deepfakes and Deskilling in Healthcare continue to grow as healthcare systems rely more heavily on automation.
Deepfakes and Trust

Deepfakes are already muddying medical advice. Picture a patient who sees a video of a respected rheumatologist endorsing a miracle cure — the doctor is real, the video fake. That kind of disinformation makes real medical conversations heavier. And when trust frays, every clinical interaction feels the strain. This is one of the most alarming aspects of AI Deepfakes and Deskilling in Healthcare.
This isn’t a daily crisis yet. But it’s a growing crack. Deepfakes can mimic a physician’s voice to give false orders, forge radiology reports, or spread lies during an outbreak. The damage to public trust isn’t easy to measure, but it compounds. As a result, AI Deepfakes and Deskilling in Healthcare is becoming a critical issue for hospitals and regulators alike.
The Deskilling Worry
The 74% figure from the survey isn’t surprising to anyone who’s seen a resident reach for a calculator before estimating a dose, or a nurse hesitate to use a manual cuff. The tools don’t cause instant incompetence, but the fear isn’t imaginary. Much of the debate around AI Deepfakes and Deskilling in Healthcare centers on whether clinicians may gradually lose essential skills.
Dr. Peter Bonis, the company’s chief medical officer, pointed to research in other fields showing that heavy reliance on automated systems can interfere with developing and retaining core skills. You can learn a task wrong from the start, or lose abilities you once had. In medicine, that’s terrifying. The counterargument — and I lean this way — is that we can design workflows that keep us engaged. Use AI to handle the cognitive clutter: collating articles, scribbling notes, flagging abnormal labs. But then formulate a diagnosis without peeking at the AI’s suggestion first. That feels uncomfortable, but it keeps your own pattern-recognition circuits firing. Finding that balance is essential in addressing AI Deepfakes and Deskilling in Healthcare.
If you ask a resident to list differentials before looking at the model’s output, she might hesitate, then give a reasoned list that matches the AI’s top two. She just needed the silence to trust herself. That’s the muscle we can’t let atrophy. Preserving clinical judgment remains one of the biggest challenges associated with AI Deepfakes and Deskilling in Healthcare.
AI adoption surges, but providers worry about deskilling
Hallucinations and Blind Trust
About three-quarters of clinicians in the survey said hallucinations — when AI makes up convincing but false information — are a major concern. And 73% were confident they could spot those errors. That sounds reassuring until you consider that one in four clinicians wasn’t sure they could. In a busy hospital, that’s a lot of potential missteps. These risks further highlight why AI Deepfakes and Deskilling in Healthcare deserves serious attention.
Even the confident ones may overestimate their ability. An AI summary can cite a single well-designed study with perfect formatting, then miss three others that point to a completely different clinical recommendation. If you don’t already know the literature, you’d never catch it. The real trap is not just outright fabrications, but the authoritative tone that lulls you into nodding along. Every unchecked output makes the next one harder to verify. Experts warn that AI Deepfakes and Deskilling in Healthcare could become more problematic if blind trust in automated systems replaces independent clinical review.
As hospitals continue expanding their use of AI, the conversation around AI Deepfakes and Deskilling in Healthcare will remain central to discussions about patient safety, medical ethics, and the future of clinical decision-making. Addressing AI Deepfakes and Deskilling in Healthcare requires thoughtful governance, continuous training, and a commitment to keeping human expertise at the heart of healthcare.

A way forward
The technology isn’t going away, and honestly, we shouldn’t want it to. It can reduce burnout. It spots patterns in mountains of data. It gives back precious minutes with patients. But staying sharp demands intention.
For clinicians: Treat AI-generated output like a well-meaning but sleep-deprived intern — check its work. Do your core reasoning first, then look at what the model suggests. If you use a scribe tool, read every note you sign. Malpractice doesn’t accept “the bot wrote it” as a defense.
For patients: Be deeply skeptical of medical advice on social media or video platforms, especially if a celebrity doctor says something shocking. Use trusted sources for medication information — not the first chatbot result. More than half of patients already research side effects via AI; ask a real doctor if something sounds off.
For hospitals and health systems: The survey showed only 27% of clinicians knew how their workplace was addressing AI governance. That’s a dangerous gap. Institutions need clear, published policies on what tools are approved, how to verify accuracy, and who bears responsibility when things go wrong. Training shouldn’t just be about how to click the button, but when not to click it.
The next time an AI tool saves you 15 minutes, use those minutes to think more deeply about the patient, not to scroll your phone. That’s how we keep our skills where they belong. But until that 27% figure climbs, the space between the technology we use and the safeguards we have will only widen.









Post Comment